Gouré is over 1,000 kilometres from Niamey. To get there from the Nigerien capital, it takes two days by car, crossing the country, passing Zinder, and heading deep into an area where dirt tracks replace tarmac roads. And it is there, in the Gouré health district, that the mHealth platform recently chose to demonstrate that it is a digital health tool designed for extreme conditions.
Designed for the field, not the laboratory
mHealth is not an app designed for a connected environment and then loosely adapted to African contexts. The platform was designed from the outset to operate 100% offline, without any internet connection. This is not a fallback mode. It is the standard mode.
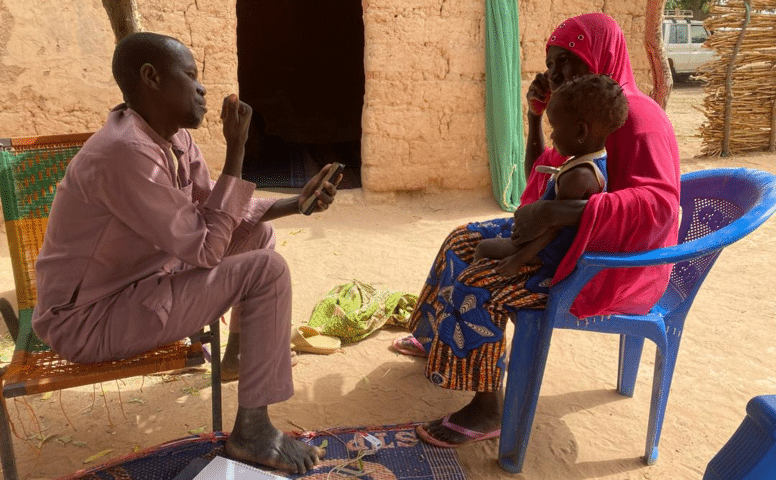
The community health worker in Gouré switches on his Android phone in the morning, opens the app and gets to work. He carries out a household survey in his area. He registers pregnant women and schedules their antenatal home visits. He looks after newborns by checking for signs of neonatal infections. They assess children under five with fever, diarrhoea or breathing difficulties using the community IMCI module, a decision tree that guides them step by step to the correct diagnosis and treatment. They monitor nutrition. They keep track of their stock of medicines.
All of this without a network. Without a connection. The phone collects the data locally, encrypts it and stores it.
And then there’s the moment when the network comes back. Sometimes when moving towards a market. Sometimes when climbing a hill. Sometimes when passing along a road with slightly better coverage. As soon as a single bar of mobile signal appears, synchronisation kicks in automatically. The data is compressed, broken down into SMS packets and sent to the central server. No internet connection is required. No need for mobile credit. The process is silent, invisible to the user. It simply does its job, and the system takes care of the rest.
It is this opportunistic synchronisation—this ability to make the most of even the slightest window of connectivity—that makes mHealth a tool ideally suited to extreme conditions.
The silent guardian of protocol
There is one benefit of mHealth that engineers may not have fully appreciated at the design stage: the clinical discipline effect.
In an environment where ongoing training is difficult to organise, where community health workers are isolated and where the nearest CSI supervisor may be hours’ walk away, the app acts as a constant safeguard. The PCIME module does more than just collect data; it sets out a specific pathway. The health worker cannot skip steps. They cannot prescribe treatment without having answered all the preliminary questions. The decision tree embedded in the phone acts, in a way, as a substitute for the absent supervisor.
For pregnant women, the antenatal care module organises appointments according to the recommended schedule. The app sends reminders about upcoming appointments, flags any delays and alerts users to warning signs. For newborns, the protocol for assessing neonatal infections is built in. For sick children, IMCI covers uncomplicated malaria, diarrhoea, pneumonia and malnutrition.
When a case exceeds the community level, the system generates a referral to the integrated health centre. This referral is recorded, time-stamped and traceable. It is no longer a piece of paper that gets lost in the post.
Making visible what was not
Before mHealth, community health data from Gouré was fed into the national health information system at a snail’s pace. The health workers’ logbooks, when they were filled in, remained in the villages. Monthly reports reached the district weeks late, incomplete, sometimes illegible, and often lost.
With the platform, every action taken by a health worker becomes actionable data. Every pregnant woman enrolled, every home visit carried out, every child treated, every referral issued. District supervisors can access this information via the mHealth Monitor dashboard as soon as the data has been synchronised.
Health centres can also report their supply needs directly via the app: shortages of antimalarial drugs, lack of oral rehydration salts for diarrhoea, or depleted stocks of amoxicillin. This flow of information, which used to rely on slow and unreliable paper-based systems, enables the CSI and the district to plan ahead rather than react to events as they unfold.
139 organisational units in one of the most challenging areas of the Sahel
The roll-out of mHealth in Gouré is not a pilot project limited to a few carefully selected villages. It is a full-scale roll-out covering 139 organisational units, including integrated health centres and community health posts.
The system is working. Data is being sent to the server. Care protocols are being followed. Pregnant women are monitored throughout their pregnancy. Sick children receive the right treatment at the right time. Patients requiring care at the CSI are referred, and this referral is tracked. Requests for supplies are reported.
If mHealth can work in Gouré – 1,000 km from the capital, with no reliable mobile network, no internet, users with limited literacy, and in a tense security situation – then it can work anywhere.
This is, in fact, confirmed by findings from other countries. In Côte d’Ivoire, an acceptability study conducted by the National Institute of Public Health and UNICEF among 280 users recorded an overall score of 4.62 out of 5, with an acceptability rate of 100%.
The invisible ones cannot wait any longer
Gouré reminds us of something fundamental. The most vulnerable populations are also the furthest removed from information systems. Women who die in childbirth in a village with no mobile network do not appear in any dashboard. Children who die from undiagnosed malaria 20 km from the nearest health centre do not trigger any alerts. These lives do not count anywhere, because no system is designed to reach them.
mHealth proves that there is another way. It shows that technology can build on whatever resources are available on the ground, however limited they may be: a mobile phone, a mobile network that comes and goes, or a community liaison who knows every family in their village. And from there, it can build a reliable, secure system that adheres to clinical protocols and transmits data.
In Gouré, every morning, community health workers switch on their mobile phones and set off to visit households. They monitor pregnant women, treat children, identify risks and issue referrals. Without the internet. Without a reliable electricity supply. Without roads. But with a tool that never lets them down, even when everything else has forgotten them.
That’s what extreme health is all about. And that’s what mHealth is all about.